
Effects of Pre-Term Birth on the Cardio-Respiratory Responses to Hypoxic Exercise in Children

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Lung Function Test
2.3. Incremental Exercise Tests
2.4. Data Processing
2.5. Statistical Analyses
3. Results
3.1. Rest
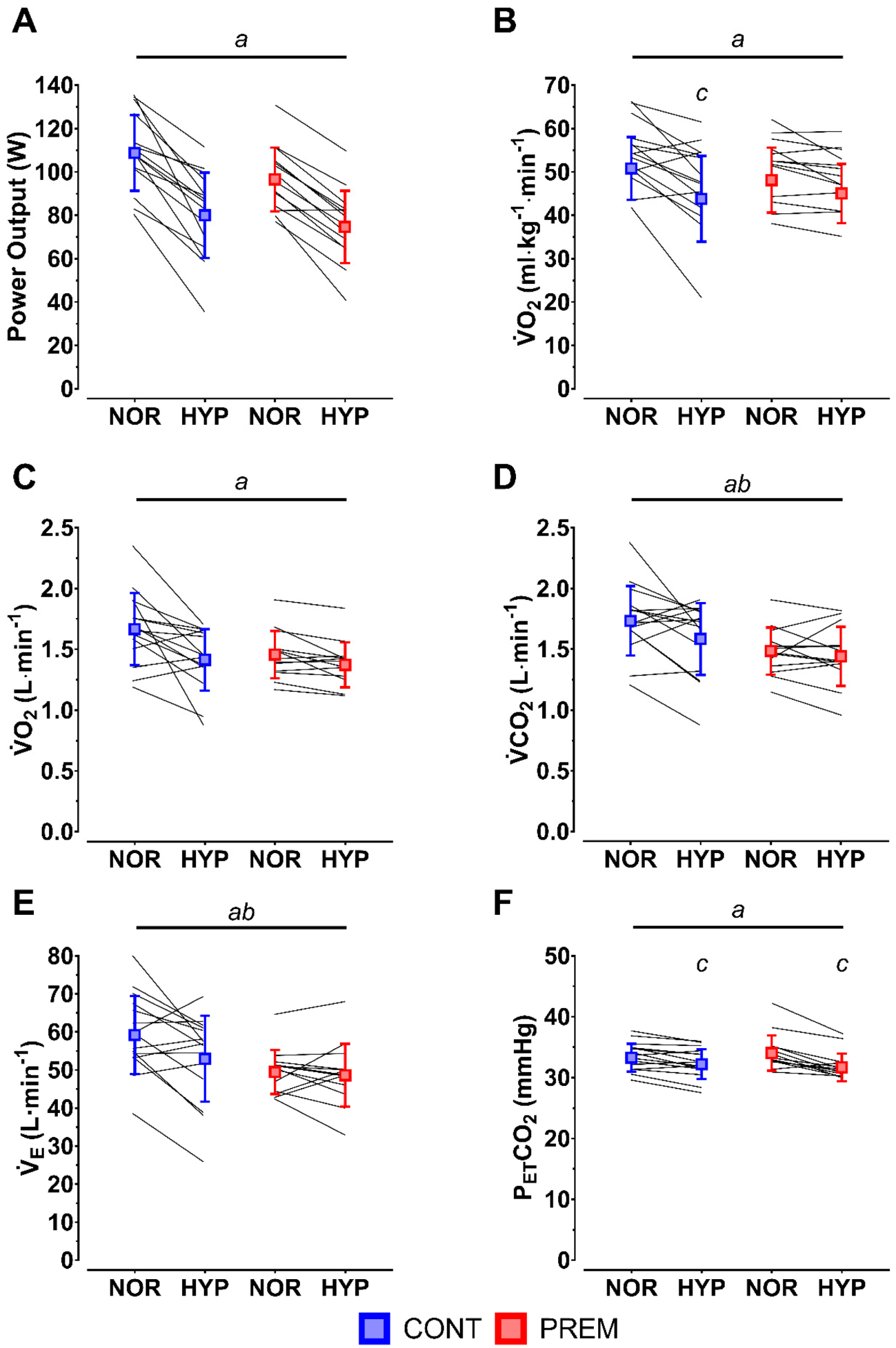
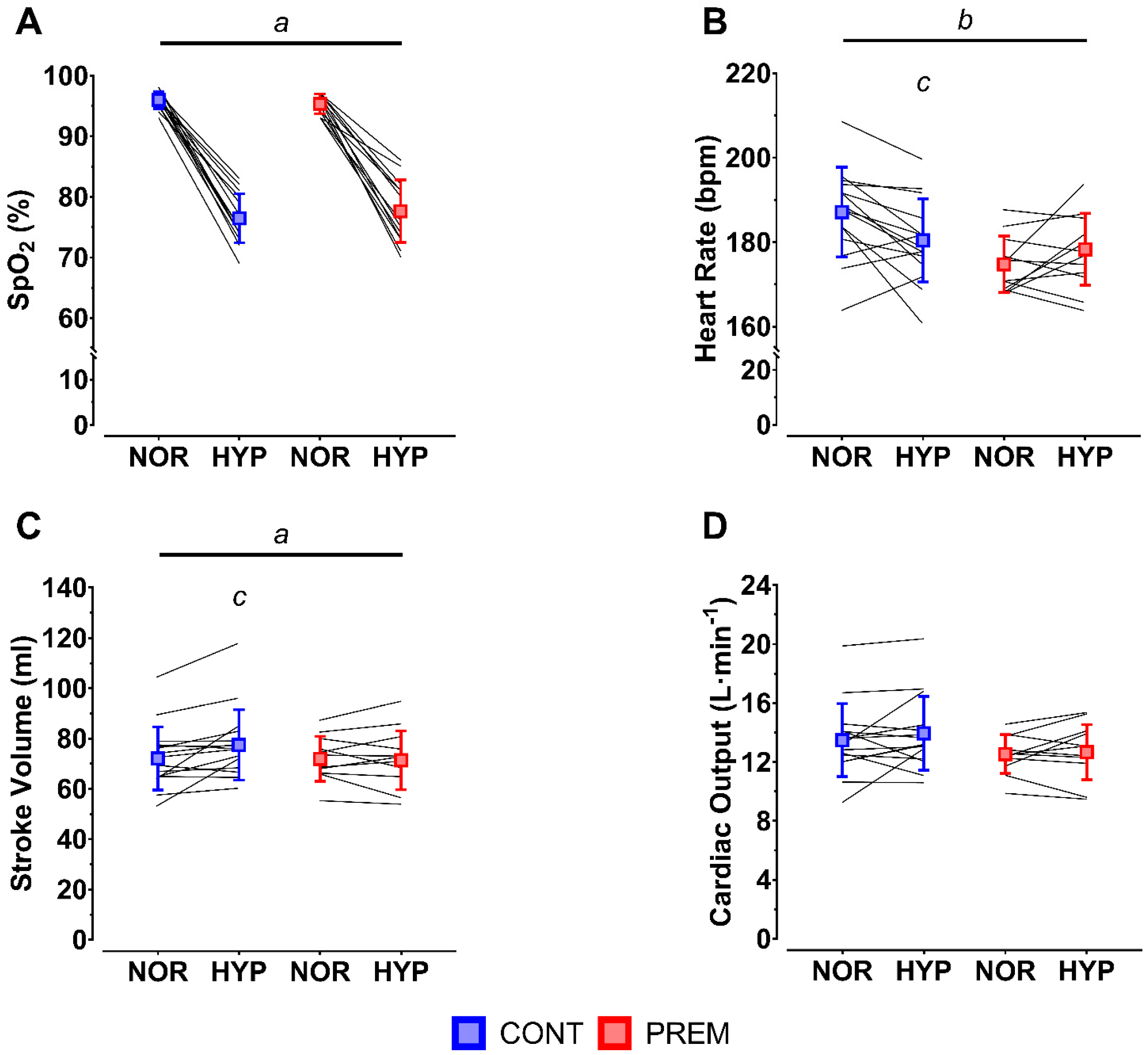
3.2. Peak
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: An updated systematic analysis with implications for the Sustainable De-velopment Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef] [Green Version]
- Duke, J.W.; Lovering, A.T. Respiratory and cardiopulmonary limitations to aerobic exercise capacity in adults born preterm. J. Appl. Physiol. (1985) 2020, 129, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Duke, J.W.; Elliott, J.E.; Laurie, S.S.; Beasley, K.M.; Mangum, T.S.; Hawn, J.A.; Gladstone, I.M.; Lovering, A.T. Pulmonary gas exchange efficiency during exercise breathing normoxic and hypoxic gas in adults born very preterm with low diffusion capacity. J. Appl. Physiol. (1985) 2014, 117, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Narang, I.; Bush, A.; Rosenthal, M. Gas Transfer and Pulmonary Blood Flow at Rest and during Exercise in Adults 21 Years after Preterm Birth. Am. J. Respir. Crit. Care 2009, 180, 339–345. [Google Scholar] [CrossRef]
- Svedenkrans, J.; Henckel, E.; Kowalski, J.; Norman, M.; Bohlin, K. Long-term impact of preterm birth on exercise capacity in healthy young men: A national population-based cohort study. PLoS ONE 2013, 8, e80869. [Google Scholar] [CrossRef]
- Bates, M.L.; Farrell, E.T.; Eldridge, M.W. Abnormal ventilatory responses in adults born prematurely. N. Engl. J. Med. 2014, 370, 584–585. [Google Scholar] [CrossRef] [Green Version]
- Debevec, T.; Pialoux, V.; Millet, G.P.; Martin, A.; Mramor, M.; Osredkar, D. Exercise Overrides Blunted Hypoxic Ventilatory Response in Prematurely Born Men. Front. Physiol. 2019, 10, 437. [Google Scholar] [CrossRef]
- O’Dea, C.A.; Logie, K.; Wilson, A.C.; Pillow, J.J.; Murray, C.; Banton, G.; Simpson, S.J.; Hall, G.L.; Maiorana, A. Lung ab-normalities do not influence aerobic capacity in school children born preterm. Eur. J. Appl. Physiol. 2021, 121, 489–498. [Google Scholar] [CrossRef]
- MacLean, J.E.; DeHaan, K.; Fuhr, D.; Hariharan, S.; Kamstra, B.; Hendson, L.; Adatia, I.; Majaesic, C.; Lovering, A.T.; Thompson, R.B.; et al. Altered breathing mechanics and ventilatory response during exercise in children born extremely preterm. Thorax 2016, 71, 1012–1019. [Google Scholar] [CrossRef] [Green Version]
- Joshi, S.; Wilson, D.G.; Kotecha, S.; Pickerd, N.; Fraser, A.G.; Kotecha, S. Cardiovascular function in children who had chronic lung disease of prematurity. Arch. Dis. Child.-Fetal Neonatal Ed. 2014, 99, F373–F379. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.M.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Fick, A. Über die Messung des Blutquantums in den Herzventrikeln. In Proceedings of the Verhandlungen der Physikalisch-medizinische Gesellschaft zu Würzburg, Würzburg, Germany. 1870, pp. 16–17. Available online: https://digitalesammlungen.uni-weimar.de/viewer/metadata/lit26189/1/ (accessed on 8 November 2021).
- Kuipers, H.; Verstappen, F.T.J.; Keizer, H.A.; Geurten, P.; van Kranenburg, G. Variability of Aerobic Performance in the Laboratory and Its Physiologic Correlates. Int. J. Sports Med. 1985, 6, 197–201. [Google Scholar] [CrossRef]
- Maxwell, S.E.; Delaney, H.D. Designing Experiments and Analyzing Data: A Model Comparison Perspective; Wadsworth: Belmont, CA, USA, 1990; p. 902. ISBN 978-053-410-374-3. [Google Scholar]
- Filippone, M.; Bonetto, G.; Corradi, M.; Frigo, A.C.; Baraldi, E. Evidence of unexpected oxidative stress in airways of adolescents born very pre-term. Eur. Respir. J. 2012, 40, 1253–1259. [Google Scholar] [CrossRef]
- Kumari, S.; Barton, G.P.; Goss, K.N. Increased mitochondrial oxygen consumption in adult survivors of preterm birth. Pediatr. Res. 2021, 90, 1147–1152. [Google Scholar] [CrossRef]
- Calder, N.A.; Williams, B.A.; Smyth, J.; Boon, A.W.; Kumar, P.; Hanson, M.A. Absence of ventilatory responses to alternating breaths of mild hypoxia and air in infants who have had bronchopulmonary dysplasia: Implications for the risk of sudden infant death. Pediatr. Res. 1994, 35, 677–681. [Google Scholar] [CrossRef] [Green Version]
- Katz-Salamon, M.; Jónsson, B.; Lagercrantz, H. Blunted peripheral chemoreceptor response to hyperoxia in a group of infants with bronchopulmonary dysplasia. Pediatr. Pulmonol. 1995, 20, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.J.; Di Fiore, J.M.; Walsh, M.C. Hypoxic Episodes in Bronchopulmonary Dysplasia. Clin. Perinatol. 2015, 42, 825–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Fiore, J.M.; Martin, R.J.; Gauda, E.B. Apnea of prematurity—Perfect storm. Respir. Physiol. Neurobiol. 2013, 189, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Vrijlandt, E.J.L.E.; Gerritsen, J.; Boezen, H.M.; Grevink, R.G.; Duiverman, E.J. Lung function and exercise capacity in young adults born prematurely. Am. J. Respir. Crit. Care Med. 2006, 173, 890–896. [Google Scholar] [CrossRef] [PubMed]
- Farrell, E.T.; Bates, M.L.; Pegelow, D.F.; Palta, M.; Eickhoff, J.C.; O’Brien, M.J.; Eldridge, M.W. Pulmonary Gas Exchange and Exercise Capacity in Adults Born Preterm. Ann. Am. Thorac Soc. 2015, 12, 1130–1137. [Google Scholar] [CrossRef]
- Faiss, R.; Pialoux, V.; Sartori, C.; Faes, C.; Dériaz, O.; Millet, G.P. Ventilation, oxidative stress, and nitric oxide in hypobaric versus normobaric hypoxia. Med. Sci. Sports Exerc. 2013, 45, 253–260. [Google Scholar] [CrossRef]
- Johnson, B.D.; Padilla, J.; Wallace, J.P. The exercise dose affects oxidative stress and brachial artery flow-mediated dilation in trained men. Eur. J. Appl. Physiol. 2012, 112, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Debevec, T.; Millet, G.P.; Pialoux, V. Hypoxia-Induced Oxidative Stress Modulation with Physical Activity. Front. Physiol. 2017, 8, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, A.; Millet, G.P.; Osredkar, D.; Mramor, M.; Faes, C.; Gouraud, E.; Debevec, T.; Pialoux, V. Effect of pre-term birth on oxidative stress responses to normoxic and hypoxic exercise. Redox Biol. 2020, 32, 101497. [Google Scholar] [CrossRef] [PubMed]
- Millet, G.P.; Vleck, V.E.; Bentley, D.J. Physiological differences between cycling and running: Lessons from triathletes. Sports Med. 2009, 39, 179–206. [Google Scholar] [CrossRef] [PubMed]
- Mourot, L. Limitation of Maximal Heart Rate in Hypoxia: Mechanisms and Clinical Importance. Front. Physiol. 2018, 9, 972. [Google Scholar] [CrossRef] [Green Version]
- Kapus, J.; Mekjavic, I.B.; McDonnell, A.C.; Ušaj, A.; Vodičar, J.; Najdenov, P.; Jakovljević, M.; Jaki Mekjavić, P.; Žvan, M.; Debevec, T. Cardiorespiratory Responses of Adults and Children during Normoxic and Hypoxic Exercise. Int. J. Sports Med. 2017, 38, 627–636. [Google Scholar] [CrossRef] [Green Version]
- Ušaj, A.; Mekjavic, I.B.; Kapus, J.; McDonnell, A.C.; Jaki Mekjavic, P.; Debevec, T. Muscle Oxygenation During Hypoxic Exercise in Children and Adults. Front. Physiol. 2019, 10, 1385. [Google Scholar] [CrossRef] [Green Version]
- Siebenmann, C.; Rasmussen, P.; Sørensen, H.; Zaar, M.; Hvidtfeldt, M.; Pichon, A.; Secher, N.H.; Lundby, C. Cardiac output during exercise: A comparison of four methods. Scand. J. Med. Sci. Sports 2014, 25, e20–e27. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control | Pre-Term | |
|---|---|---|
| Age at Test (years) | 9.7 ± 0.9 | 9.5 ± 0.3 |
| Body Mass (kg) | 33.1 ± 7.1 | 30.9 ± 5.4 |
| Height (m) | 1.40 ± 0.07 | 1.39 ± 0.07 |
| Body Mass Index (kg·m−2) | 16.8 ± 2.5 | 15.8 ± 1.6 |
| Body Fat Percentage (%) | 17.7 ± 6.6 | 16.7 ± 6.0 |
| Birth weight (g) | 3270 ± 307 | 1202 ± 184 ** |
| Gestational Age (weeks) | 39.3 ± 1.3 | 29.3 ± 1.8 ** |
| FVC (L) | 2.11 ± 0.24 | 2.11 ± 0.42 |
| FVC (% predicted) | 93 ± 7 | 93 ± 10 |
| FEV1 (L) | 1.91 ± 0.25 | 1.82 ± 0.37 |
| FEV1 (% predicted) | 97 ± 9 | 93 ± 10 |
| FEV1/FVC (%) | 90.8 ± 4.1 | 86.4 ± 6.5 * |
| FEV1/FVC (% predicted) | 103 ± 5 | 99 ± 7 |
| PEF (L·min−1) | 4.24 ± 0.95 | 3.46 ± 0.89 * |
| Normoxia | Hypoxia | Anova (p-Value) | |||||
|---|---|---|---|---|---|---|---|
| Control | Pre-Term | Control | Pre-Term | Main Effect Group | Main Effect Condition | Interaction Effect Condition*Group | |
| VO2 (L·min−1) | 0.32 ± 0.07 | 0.33 ± 0.04 | 0.36 ± 0.10 | 0.38 ± 0.06 | 0.463 | 0.019 | 0.706 |
| VO2 (ml·kg−1·min−1) | 9.7 ± 1.8 | 11.0 ± 2.5 | 11.2 ± 3.6 | 12.6 ± 3.2 | 0.188 | 0.006 | 0.844 |
| VO2 (%VO2peak) | 20.3 ± 5.7 | 22.9 ± 3.8 | 25.0 ± 6.5 | 28.3 ± 7.2 | 0.104 | 0.001 | 0.832 |
| VCO2 (L·min−1) | 0.29 ± 0.06 | 0.30 ± 0.05 | 0.38 ± 0.09 | 0.40 ± 0.06 | 0.498 | <0.001 | 0.660 |
| RQ | 0.92 ± 0.07 | 0.91 ± 0.06 | 1.13 ± 0.22 | 1.08 ± 0.07 | 0.333 | <0.001 | 0.591 |
| VE (L·min−1) | 9.3 ± 2.0 | 9.6 ± 1.4 | 12.1 ± 2.8 | 13.0 ± 2.0 | 0.411 | <0.001 | 0.571 |
| VE (%VEpeak) | 16 ± 5 | 20 ± 3 | 24 ± 8 | 28 ± 7 | 0.095 | <0.001 | 0.950 |
| VT (L) | 0.47 ± 0.10 | 0.50 ± 0.13 | 0.57 ± 0.18 | 0.64 ± 0.12 | 0.292 | <0.001 | 0.503 |
| Bf (b·min−1) | 20.3 ± 4.5 | 20.2 ± 3.4 | 23.1 ± 5.4 | 21.2 ± 3.7 | 0.432 | 0.022 | 0.341 |
| SpO2 (%) | 97.6 ± 0.7 | 97.1 ± 1.2 | 88.5 ± 2.9 | 90.2 ± 4.0 | 0.431 | <0.001 | 0.126 |
| HR (bpm) | 97 ± 8 | 92 ± 11 | 107 ± 8 | 106 ± 13 | 0.355 | <0.001 | 0.394 |
| HR (%HRpeak) | 52 ± 2 | 51 ± 4 | 60 ± 5 | 59 ± 7 | 0.437 | <0.001 | 0.521 |
| SV (ml) | 55 ± 9 | 53 ± 8 | 62 ± 8 | 56 ± 7 | 0.178 | <0.001 | 0.070 |
| CO (L·min−1) | 5.4 ± 0.9 | 4.9 ± 0.7 | 6.6 ± 0.9 | 5.8 ± 0.9 | 0.040 | <0.001 | 0.380 |
| PETO2 (mmHg) | 108 ± 4 | 110 ± 3 | 61 ± 4 | 61 ± 2 | 0.720 | <0.001 | 0.337 |
| PETCO2 (mmHg) | 33 ± 2 | 33 ± 1 | 33 ± 2 | 33 ± 1 | 0.649 | 0.358 | 0.825 |
| EqO2 | 30.8 ± 4.1 | 30.1 ± 2.7 | 37.2 ± 8.4 | 34.8 ± 2.7 | 0.272 | <0.001 | 0.585 |
| EqCO2 | 32.7 ± 2.4 | 32.8 ± 1.7 | 32.6 ± 2.3 | 32.3 ± 1.6 | 0.463 | 0.019 | 0.706 |
| A-V O2 diff (%) | 5.9 ± 0.8 | 6.7 ± 1.2 | 5.4 ± 1.6 | 6.6 ± 1.7 | 0.188 | 0.006 | 0.844 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Narang, B.J.; Manferdelli, G.; Kepic, K.; Sotiridis, A.; Osredkar, D.; Bourdillon, N.; Millet, G.P.; Debevec, T. Effects of Pre-Term Birth on the Cardio-Respiratory Responses to Hypoxic Exercise in Children. Life 2022, 12, 79. https://doi.org/10.3390/life12010079
Narang BJ, Manferdelli G, Kepic K, Sotiridis A, Osredkar D, Bourdillon N, Millet GP, Debevec T. Effects of Pre-Term Birth on the Cardio-Respiratory Responses to Hypoxic Exercise in Children. Life. 2022; 12(1):79. https://doi.org/10.3390/life12010079
Chicago/Turabian StyleNarang, Benjamin J., Giorgio Manferdelli, Katja Kepic, Alexandros Sotiridis, Damjan Osredkar, Nicolas Bourdillon, Grégoire P. Millet, and Tadej Debevec. 2022. "Effects of Pre-Term Birth on the Cardio-Respiratory Responses to Hypoxic Exercise in Children" Life 12, no. 1: 79. https://doi.org/10.3390/life12010079